The rationale for determining the minimum ventilation rate requirements is based on two main aspects.
First, we consider the effect of air-change rate on decay of droplet nuclei concentration. shows the calculated pollutant concentration decay with different ventilation rates in fully mixed isolation rooms, assuming the pollutant concentration in outdoor air is 0 and there is no source in the enclosed space according to the simple concentration decay equation. The table shows that there is 7-fold dilution within 10 minutes at 12 air changes per hour (ACH), 20-fold dilution within 10 minutes at 18 ACH and 54-fold dilution within 10 minutes at 24 ACH.
Decay of droplet nuclei concentration in an isolation room for different ventilation rates and duration of time.
Second, we use mathematical modelling of infection risk using the Wells–Riley equation to estimate the effect of ventilation rate on infection probability for known airborne diseases. The Wells–Riley equation was developed for predicting the probability of airborne disease transmission.
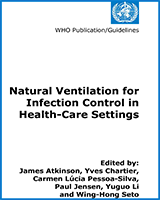
We can calculate the infection risk in an enclosed room with different ventilation rates and quanta generations. The calculated results are shown in when we assume one infector entering an enclosed room with a dimension of 6 m × 6.7 m × 2.7 m over a period of one hour. The cross-infection risk of airborne-transmitted diseases decreases when the ventilation rate increases, especially for the low quanta-generation rate, while the actual reported average quanta-generation rate of different airborne diseases is low.
Infection risk with 15 minutes exposure with different ventilation rates and quanta generation for an infector entering an enclosed space with a dimension 6 m × 6.7 m × 2.7 m.
The benefits of using higher ventilation rates are also obvious. In clinical situations, where droplet nuclei are an important mode of disease transmission, the average quanta production rates in clinical patients not undergoing aerosol-generating procedures is usually <1 quanta/minute, and between 4–6 quanta/minute for bronchoscopy. With a quanta production rate of 10 quanta/minute, the estimated risk of infection with 15 minutes of exposure in a room with 12 ACH is 4%, and with 24 ACH is 2%, which illustrates the importance of adequate ventilation.